A droopy eyelid that develops gradually over years is usually a cosmetic concern. A droopy eyelid that appears suddenly is a different conversation. The difference between the two is not subtle, and recognizing it matters because some causes of acute ptosis (the medical term for a drooping upper eyelid) require urgent evaluation. Here is how to tell them apart and when to seek care.
Ptosis refers to the upper eyelid sitting lower than it should, partially or fully covering the pupil. It can affect one eye or both. The cause depends on which structure is involved: the muscle that lifts the eyelid (the levator), the nerves that supply that muscle, the small Mueller's muscle that contributes to eyelid elevation, or the tissues surrounding the eye.
Most ptosis falls into two broad categories. Aponeurotic ptosis (also called involutional ptosis) is the slow, age-related form. It develops over years as the levator muscle's attachment to the eyelid stretches. Acute ptosis is the sudden form, and the underlying cause can range from completely benign to genuinely urgent.
A few causes of acute ptosis require evaluation within hours, not days. Per the American Academy of Ophthalmology, several presentations should trigger immediate medical attention:
A droopy eyelid accompanied by a blown (dilated) pupil on the same side. This pattern can indicate compression of the third cranial nerve, sometimes from an aneurysm of the posterior communicating artery. This is a neurosurgical emergency.
A droopy eyelid with a smaller pupil on the affected side, sometimes with reduced sweating on that side of the face. This is the classic triad of Horner's syndrome, which can be caused by carotid artery dissection, tumors, or other vascular causes. New-onset Horner's syndrome with neck pain or headache requires emergency imaging to rule out a dissection.
A droopy eyelid that fluctuates, gets worse with use, and improves with rest. This pattern, sometimes worsened in the evening or after reading, can be a sign of myasthenia gravis. Myasthenia is often called "the great imitator" because it can affect just the eyelid muscles initially before involving other muscle groups.
A droopy eyelid accompanied by sudden weakness on one side of the body, slurred speech, facial drooping, or vision changes. These are stroke symptoms. Call 911 immediately.
A droopy eyelid following a head injury, even a mild one. New ptosis after trauma needs evaluation to rule out nerve injury or orbital fracture.
If any of these patterns describe what you are experiencing, do not wait. Go to an emergency department or call 911.

Not every case of acute ptosis is an emergency. Some causes are uncomfortable but generally not dangerous. They still deserve evaluation, just not in the next hour.
Common less-urgent causes include:
Inflammation or swelling around the eyelid (a stye, severe blepharitis, or contact dermatitis) that pushes the eyelid down temporarily. Once the swelling resolves, eyelid position usually returns to normal.
Recent eye surgery, including cataract surgery, which can occasionally cause a temporary or longer-lasting ptosis from stretching of the levator during the procedure. This often improves over weeks to months.
A complication of cosmetic injections, particularly Botox, where diffusion of the neurotoxin to the levator muscle causes a temporary droop. This typically resolves over four to eight weeks as the effect wears off.
Bell's palsy, a temporary weakness of the facial nerve that causes drooping of one side of the face including the eyelid. Bell's palsy is usually self-limiting but should be evaluated by a physician within 72 hours of onset to discuss treatment options.
If you fall into one of these categories, an evaluation by an ophthalmologist or oculoplastic surgeon within a few days is appropriate. Same-day care is not required, but do not put it off for weeks.
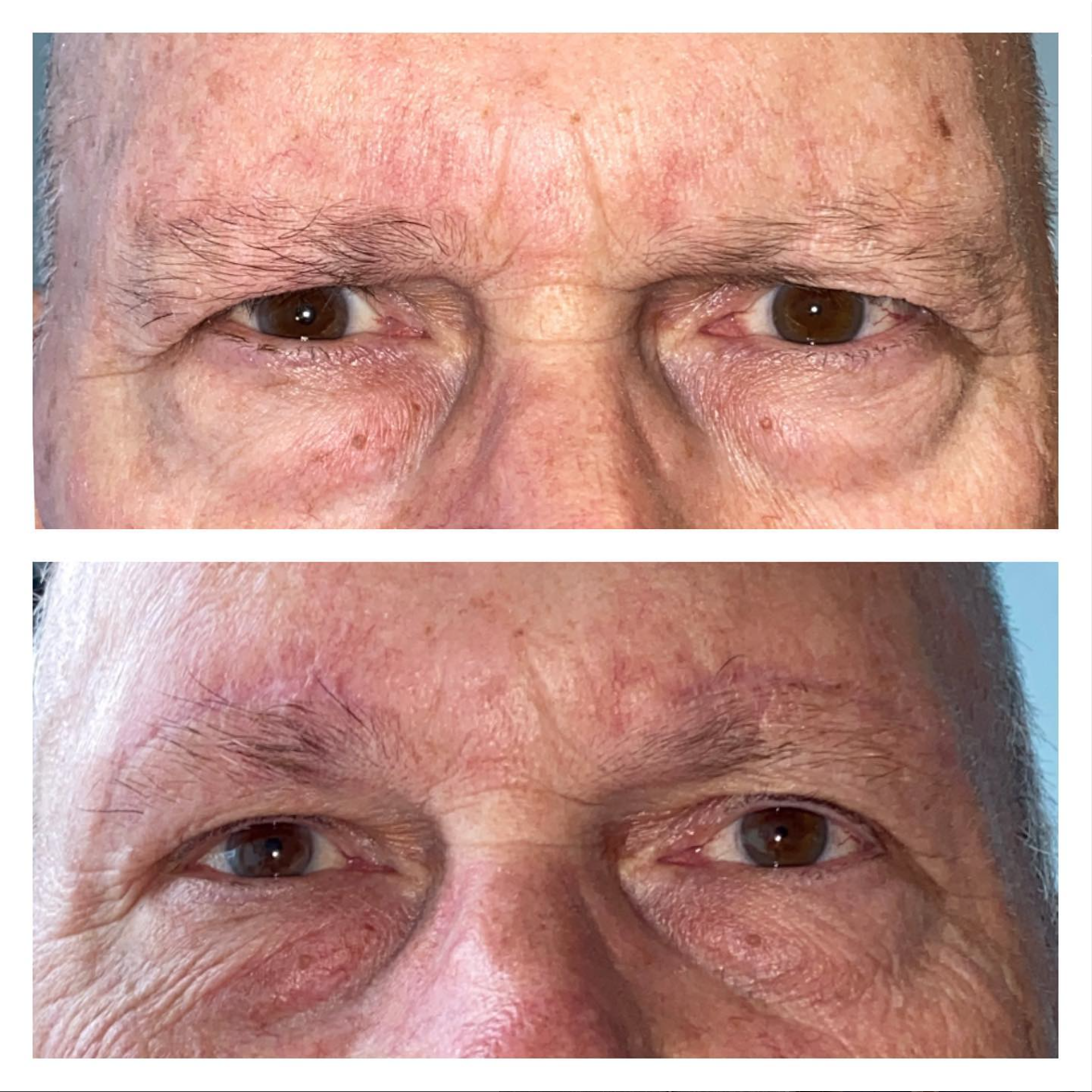
The most common cause of a droopy upper eyelid in adults is involutional or aponeurotic ptosis. This is the slow form. It develops over years, sometimes decades, as the levator muscle's connection to the eyelid stretches and weakens. It often affects both eyes, though usually not symmetrically.
Patients with age-related ptosis often describe the same set of symptoms: tired-looking eyes, a feeling of heaviness in the upper eyelids by the end of the day, the need to raise the eyebrows or tilt the head back to see clearly, and difficulty with peripheral or upper field vision.
Age-related ptosis is not an emergency, but it is correctable. Treatment is usually a surgical repair of the levator (called levator advancement or levator resection), performed under local anesthesia or light sedation, with a recovery similar to other eyelid procedures. In many cases, when ptosis significantly affects vision, the procedure may be partially covered by insurance.
If you have noticed gradual drooping over months or years, schedule a consultation with an oculoplastic surgeon. The evaluation includes measurements of eyelid position, levator function, and visual field testing if insurance coverage may be relevant.
A focused ptosis evaluation looks at several specific things: the height of the eyelid relative to the pupil, how much the eyelid moves when the levator muscle contracts (called levator function), the depth and position of the eyelid crease, the strength of the surrounding muscles, and the function of the pupils and eye movements.
The history matters as much as the exam. When did this start? Did it appear overnight or gradually? Does it fluctuate? Are there other neurological symptoms? Has there been recent eye surgery, head trauma, or new medications?
That combination of history and exam usually points clearly to either an aging-related cause that can be discussed at the patient's pace or an acute cause that needs urgent imaging or referral.
If you have no other neurological symptoms (no pupil changes, no weakness elsewhere, no vision changes, no headache or neck pain), an urgent visit to an ophthalmologist or oculoplastic surgeon within 24 to 48 hours is reasonable. Any new neurological symptom, however, should send you to the ER immediately.
Stress alone is not a typical cause. However, fatigue can make existing mild ptosis more noticeable, and stress sometimes accompanies conditions like myasthenia gravis or migraine that can affect eyelid position. If a droop persists, it is worth evaluating.
Age-related ptosis usually progresses slowly. Acute ptosis depends entirely on the cause. The right next step is identifying which type you are dealing with.
Dr. David Z. Gay is a board-certified ophthalmologist with fellowship training in oculofacial plastic and reconstructive surgery, and ptosis evaluation and repair are core to the practice. If you have noticed a sudden change in your eyelid position with any concerning neurological symptoms, please go to an emergency department first. If your situation is non-urgent and you would like an evaluation for ptosis, schedule a consultation online or call our Dripping Springs office at 512-607-6884.


13830 Sawyer Ranch Road
Suite 201 Dripping Springs,
TX 78620
Inside Howerton Eye
4282 Farm to Market 1626
Suite 200
Kyle, TX 78640
Inside VIEW Temple
221 Paloma Drive
Temple, TX 76502
Inside New Braunfels Vision Center
1439 Hanz Drive
New Braunfels, TX 78130




